60 yr old male with dov in both eyes ,hypertension,bronchial asthma
I am P.Durga Bhavani, 5th sem medical student. This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CONSENT AND DE-IDENTIFICATION :
The patient and the attenders have been adequately informed about this documentation and privacy of the patient is being entirely conserved. No identifiers shall be revealed throughout this piece of work whatever.
Chief Complaints:
A 60 Male farmer by occupation resident of suryapet came to OPD with chief Complaints of diminution of vision of both eyes since 3-4 months.
History of Present Illness:
Patient was apparently asymptomatic 3 months ago then developed DOV in both eyes which is insidious in onset and gradually progressive.
No c/o chest pain, palpitations,SOB, orthopena,PND,pedal edema, decreased urine output.
Past history:
-K/c/o asthma since 6 years on Ipratropium bromide and Levosulphate ,Rotacap inhalers
-H/o pulmonary TB 20 years ago
-Not a k/c/o CAD,CVA,asthma, epilepsy.
Surgical history: no surgical history
Personal History:
- married
- decreased appetite
- mixed diet
- Sleep adequate
- regular bowels
- abnormal micturition
- no known allergies
- no addictions
Family History: not significant
General Examination:
I have examined the patient after taken prior consent and informing the patient in the presence of a female attendant. The examination was done in both supine and sitting position in a well lit room.
- patient was conscious, coherent and cooperative
- well oriented to time and space
- well built and adequately nourished
- no pallor
- no icterus
- no cyanosis
- no clubbing of fingers
- no lymphadenopathy
- no edema
- no malnutrition
- no dehydration
Vitals:
- Temperature: afebrile
- Pulse: 82 beats/min
- RR: 16 cycles/min
- BP: 140/80 mm Hg measured in right arm in supine position
Systemic Examination:
Respiratory System
- upper respiratory tract : oral cavity, nose & oropharynx appear normal
- chest is bilaterally symmetrical
- respiratory movements appear equal on both sides and of thoracoabdominal type
- position of trachea : central
- vesicular breath sounds : present
- no wheeze
Cardiovascular System:
Inspection :
- shape of chest : elliptical
- no engorged veins, scars, visible pulsations
Palpation :
-Apex beat can be palpable in 5th intercostal space
- no cardiac thrills
Auscultation :
- S1,S2 are heard
- no murmurs
Abdomen:
- shape: scaphoid
- no tenderness
- no palpable mass
- no bruits
- no free fluid
- hernias orifices: normal
- liver: not palpable
- spleen : not palpable
- no bowel sounds
- genitals: normal
- speculum examination : normal
- P/R examination : normal
Central Nervous System:
- conscious
- normal speech
- no neck stiffness
- no Kerning's sign
- cranial nerves: normal
- sensory : normal
- motor: normal
- reflexes: all present bilaterally
- finger nose in coordination: not seen
- knee heel in coordination: not seen
- gait: normal
Investigations:
Ocular examination:

Hemogram:
Hb:13.0
TLC:10,700
N/L/E/M: 73/14/3/10
PLT:3.26
RFT:
BU:20
SC:0.8
Na+:135
K+:4.5
Cl-:103
LFT:
TB:0.64
PB:0.19
SGOT:122
SGPT:138
ALP:291
TP:6.8
Alb:4.2
A/G:1.66
2D ECHO :
EF:6.3
Concentric LVH,No RWMA
IVC:1.12 cm collapsing
RVSP:35 mm Hg

Serology :
Negative
CXR PA view:
Right unilateral fibrosis
RS:
BAE+,VBS+,
BL Rhonchi +,inter SA,Infra SA,
IAA,AA,ICA,MA.
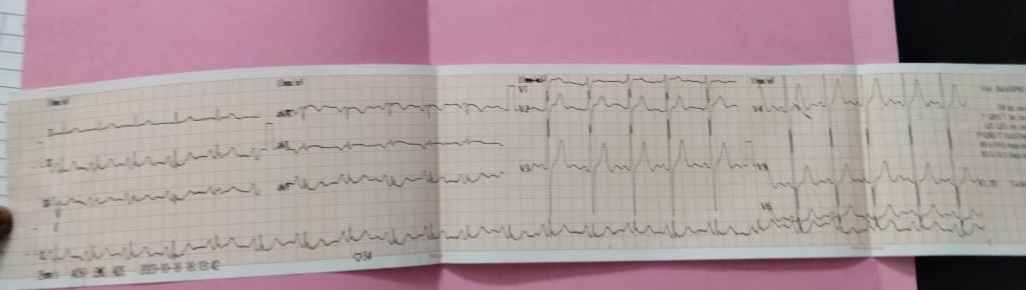
ECG:
Provisional Diagnosis:
-left eye senile mature cataract
-denovo c/o HTN
-k/c/o bronchial asthma
Medication:


